Abstract
Background: Tuberculosis (TB) remains a major public health issue in Ethiopia, with a high burden of both pulmonary and extrapulmonary TB cases. The prevalence of TB, including drug-resistant forms, continues to pose challenges, particularly in hospital settings like Dessie Comprehensive Specialized Hospital where both new and relapse cases are reported. This study aimed to determine the five-year prevalence and associated factors of MTB among TB-suspected cases at Dessie Comprehensive Specialized Hospital from 2020–2024. Method: A retrospective cross-sectional study was conducted using medical records of 1,850 TB-suspected cases. Data on socio-demographics, clinical presentation, and laboratory results (Gene-Xpert MTB/RIF) were analyzed using descriptive statistics and logistic regression. Results: The overall MTB prevalence was 23.4% (433/1,850). Significant risk factors included HIV co-infection (AOR=3.12, 95% CI: 2.34-4.16), malnutrition (AOR=2.45, 95% CI: 1.89-3.18), smoking (AOR=1.89, 95% CI: 1.32-2.71), and previous TB treatment (AOR=2.67, 95% CI: 1.95-3.65). Conclusion: The high MTB prevalence underscores the need for enhanced TB screening, particularly among high-risk groups.
Keywords
Tuberculosis, Mycobacterium Tuberculosis, Prevalence, Risk Factors, Ethiopia, Retrospective Study, HIV, Gene x Pert, Northeast, Ethiopia
1. Introduction
1.1. Back Ground
Tuberculosis, Tuberculosis, caused by
Mycobacterium tuberculosis, is one of the top 10 causes of death globally and the leading infectious killer, especially in low- and middle-income countries
| [1] | World Health Organization. Global tuberculosis report 2023. Geneva: World Health Organization; 2023. Licence: CC BY-NC-SA 3.0 IGO. |
| [2] | Wondwossen F, Tsegaye W, Abate E. Prevalence and risk factors for multidrug-resistant tuberculosis in previously treated and new cases in Ethiopia. Infect Drug Resist. 2019; 12: 2151–8. https://doi.org/10.2147/IDR.S210344 |
[1, 2]
. In 2022, Ethiopia reported an estimated TB incidence of 126 per 100,000 population, with approximately 156,000 new cases and 21,000 TB-related deaths
| [3] | World Health Organization. Global tuberculosis report 2022. Geneva: World Health Organization; 2022. Licence: CC BY-NC-SA 3.0 IGO. |
| [4] | World Health Organization. Automated real-time nucleic acid amplification technology for rapid and simultaneous detection of tuberculosis and rifampicin resistance: Xpert MTB/RIF assay for the diagnosis of pulmonary and extrapulmonary TB in adults and children – policy update 2013. Geneva: World Health Organization; 2013. WHO/HTM/TB/2013.16. |
[3, 4]
. The country ranks 15th globally and 7th in Africa for TB burden
| [5] | World Health Organization. The End TB Strategy: Global strategy and targets for tuberculosis prevention, care and control after 2015. Geneva: World Health Organization; 2015. WHO/HTM/TB/2015.19. |
[5]
. The Amhara region, where Dessie Hospital is located, consistently reports high TB case numbers, with a significant proportion of rifampicin-resistant TB (RR-TB) and multidrug-resistant TB (MDR-TB)
| [6] | Abate E, Bekele A, Birlie B, Berisa S, Deribe T, Tsegaye G, et al. Multidrug-resistant tuberculosis in Ethiopian settings and its association with previous history of anti-tuberculosis treatment: a systematic review and meta-analysis. BMC Pulm Med. 2018; 18(1): 24. https://doi.org/10.1186/s12890-018-0588-2 |
| [7] | Mekonnen F, Tessema B, Moges F, Mengistu G, Mengistu Y, Dagnew M. Multidrug resistant tuberculosis: prevalence and risk factors in districts of Metema and West Armachiho, Northwest Ethiopia. BMC Infect Dis. 2015; 15: 461.
https://doi.org/10.1186/s12879-015-1191-2 |
[6, 7]
. HIV co-infection, previous TB treatment, and socio-economic factors exacerbate TB transmission and complicate treatment outcomes
| [1] | World Health Organization. Global tuberculosis report 2023. Geneva: World Health Organization; 2023. Licence: CC BY-NC-SA 3.0 IGO. |
| [6] | Abate E, Bekele A, Birlie B, Berisa S, Deribe T, Tsegaye G, et al. Multidrug-resistant tuberculosis in Ethiopian settings and its association with previous history of anti-tuberculosis treatment: a systematic review and meta-analysis. BMC Pulm Med. 2018; 18(1): 24. https://doi.org/10.1186/s12890-018-0588-2 |
[1, 6]
. The introduction of Gene-Xpert MTB/RIF assay has improved rapid diagnosis and detection of rifampicin resistance, yet challenges remain in diagnostic coverage and treatment adherence
| [4] | World Health Organization. Automated real-time nucleic acid amplification technology for rapid and simultaneous detection of tuberculosis and rifampicin resistance: Xpert MTB/RIF assay for the diagnosis of pulmonary and extrapulmonary TB in adults and children – policy update 2013. Geneva: World Health Organization; 2013. WHO/HTM/TB/2013.16. |
[4]
.
In Ethiopia, several studies have assessed the prevalence of TB among different populations and hospital attendees. However, limited data exist on the prevalence of TB burden among TB suspected patients, particularly at Dessie Comprehensive Specialized Hospital. This study aims to fill this gap by determining the prevalence of TB and identifying associated risk factors. The findings will inform public health interventions focused on screening, prevention, and management strategies.
Therefore, this study aims to assess the Prevalence of TB among TB suspected patients at Dessie Comprehensive Specialized Hospital, Northeast Ethiopia.
1.2. Literature Review
The global efforts to eradicate TB face substantial obstacles, particularly in high-burden countries like Ethiopia. According to the World Health Organization (WHO), TB remains a major public health threat, driven by factors such as HIV co-infection, malnutrition, poverty, and weak health systems
| [1] | World Health Organization. Global tuberculosis report 2023. Geneva: World Health Organization; 2023. Licence: CC BY-NC-SA 3.0 IGO. |
| [2] | Wondwossen F, Tsegaye W, Abate E. Prevalence and risk factors for multidrug-resistant tuberculosis in previously treated and new cases in Ethiopia. Infect Drug Resist. 2019; 12: 2151–8. https://doi.org/10.2147/IDR.S210344 |
[1, 2]
. The WHO End TB Strategy aims for a 90% reduction in TB deaths and an 80% reduction in the TB incidence rate by 2030, emphasizing early diagnosis and universal drug susceptibility testing
| [5] | World Health Organization. The End TB Strategy: Global strategy and targets for tuberculosis prevention, care and control after 2015. Geneva: World Health Organization; 2015. WHO/HTM/TB/2015.19. |
[5]
.
1.2.1. TB Burden and Drug Resistance in Ethiopia
Ethiopia is one of the 30 high TB burden countries, with regional heterogeneity in incidence and prevalence
| [3] | World Health Organization. Global tuberculosis report 2022. Geneva: World Health Organization; 2022. Licence: CC BY-NC-SA 3.0 IGO. |
[3]
. The first national TB prevalence survey highlighted a substantial burden, particularly in Amhara and Oromia regions
| [9] | Kebede AH, Alebachew Z, Tsegaye F, et al. The first population-based national tuberculosis prevalence survey in Ethiopia, 2010–2011. Int J Tuberc Lung Dis. 2014; 18(6): 635–9. https://doi.org/10.5588/ijtld.13.0821 |
[9]
. Furthermore, drug-resistant TB (DR-TB), including MDR-TB, poses a growing threat. Systematic reviews of Ethiopian settings have found that previous history of anti-TB treatment is the strongest independent predictor of acquiring MDR-TB
| [6] | Abate E, Bekele A, Birlie B, Berisa S, Deribe T, Tsegaye G, et al. Multidrug-resistant tuberculosis in Ethiopian settings and its association with previous history of anti-tuberculosis treatment: a systematic review and meta-analysis. BMC Pulm Med. 2018; 18(1): 24. https://doi.org/10.1186/s12890-018-0588-2 |
| [8] | Ethiopia Central Statistical Agency. Population and Housing Census of 2007: Amhara Region [Internet]. Addis Ababa: Central Statistical Agency; 2010. |
[6, 8]
, underscoring the challenges of adherence and treatment completion. Studies in Northwest Ethiopia, geographically and socio-economically similar to the study setting, have also reported high MDR-TB prevalence among previously treated patients
| [7] | Mekonnen F, Tessema B, Moges F, Mengistu G, Mengistu Y, Dagnew M. Multidrug resistant tuberculosis: prevalence and risk factors in districts of Metema and West Armachiho, Northwest Ethiopia. BMC Infect Dis. 2015; 15: 461.
https://doi.org/10.1186/s12879-015-1191-2 |
[7]
.
1.2.2. Clinical and Socio-Demographic Risk Factors
The epidemiology of TB is inextricably linked to socio-demographic and clinical factors. The high prevalence of TB among HIV-positive individuals is well-documented, with co-infected patients having significantly increased odds of TB diagnosis due to severe immune suppression
| [10] | Dadi M, et al. Prevalence and factors associated with tuberculosis among HIV-positive adults attending a public health facility in Ethiopia. BMC Infect Dis. 2019; 19: 290. https://doi.org/10.1186/s12879-019-3890-4 |
| [15] | Mamo G, et al. The burden of TB/HIV co-infection and its associated factors in Ethiopia: a systematic review and meta-analysis. BMC Public Health. 2022; 22: 1568.
https://doi.org/10.1186/s12889-022-14002-3 |
[10, 15]
.
Furthermore, malnutrition is a critical determinant of TB progression. Undernutrition impairs cellular immunity, leading to a higher risk of developing active TB disease among those with latent infection
. Studies examining trends in Ethiopia have consistently identified age (young adults), male sex, and urban residence as key demographic risk factors
| [12] | Abera SF, et al. Trend of tuberculosis and its association with socio-demographic factors in Ethiopia: A retrospective study. Infect Dis Poverty. 2021; 10: 42.
https://doi.org/10.1186/s40249-021-00827-0 |
| [14] | Tsegaye AT, Wondifraw Z. Epidemiology and risk factors of pulmonary tuberculosis in Ethiopia: A systematic review and meta-analysis of observational studies. PLoS One. 2024; 19(1): e0297594. https://doi.org/10.1371/journal.pone.0297594 |
[12, 14]
. Males, particularly those in the economically productive age group (25-44 years), are often more mobile and may have higher rates of co-morbidities like smoking and alcohol use, further increasing their vulnerability to TB
| [13] | Zewdu MK, et al. Prevalence of tuberculosis and associated risk factors among adult populations in Ethiopia: A systematic review and meta-analysis. Syst Rev. 2022; 11: 172.
https://doi.org/10.1186/s13643-022-02052-7 |
[13]
. Smoking, in particular, has been shown to impair pulmonary clearance mechanisms, significantly elevating TB risk
.
1.2.3. Diagnostic Advancements
The introduction of rapid diagnostic tools, notably the GeneXpert MTB/RIF assay, has revolutionized TB control by enabling rapid, simultaneous detection of
M. tuberculosis and Rifampicin resistance, replacing time-consuming conventional microscopy and culture
| [4] | World Health Organization. Automated real-time nucleic acid amplification technology for rapid and simultaneous detection of tuberculosis and rifampicin resistance: Xpert MTB/RIF assay for the diagnosis of pulmonary and extrapulmonary TB in adults and children – policy update 2013. Geneva: World Health Organization; 2013. WHO/HTM/TB/2013.16. |
[4]
. Despite this advancement, optimizing diagnostic algorithms and ensuring universal access, especially in resource-limited settings like Dessie Comprehensive Specialized Hospital, remains a key challenge in mitigating the overall TB burden.
1.3. Statement of the Problem
Despite national TB control programs and improved diagnostics, Ethiopia continues to face a high TB burden with rising drug resistance. Dessie Comprehensive Specialized Hospital serves a large population in a TB endemic area, but there is limited comprehensive data on the prevalence of M. tuberculosis, rifampicin resistance, and associated risk factors over an extended period. This gap hinders targeted interventions and resource allocation. Understanding local epidemiology and factors associated with TB positivity and drug resistance is critical for improving diagnosis, treatment, and control measures.
Hence, this study designed, to assess Prevalence of TB among TB suspected patients at Dessie Comprehensive Specialized Hospital, Northeast Ethiopia.
1.4. Significance of the Study
This study was provide critical data on the burden of
Reliable data on the prevalence of *M. tuberculosis* infection and rifampicin resistance among suspected TB cases at Dessie Hospital over five years.
Identification of socio-demographic and clinical factors associated with TB infection and drug resistance.
Evidence to inform local TB control strategies, improve diagnostic algorithms, and optimize treatment protocols.
A basis for public health policy and resource prioritization in the Amhara region.
Therefore, the current study is aimed to assess the five years prevalence TB among TB suspected patients attending Dessie Comprehensive Specialized Hospital (DCSH), Northeast Ethiopia.
2. Literature Review
The global efforts to eradicate TB face substantial obstacles, particularly in high-burden countries like Ethiopia. According to the World Health Organization (WHO), TB remains a major public health threat, driven by factors such as HIV co-infection, malnutrition, poverty, and weak health systems
| [1] | World Health Organization. Global tuberculosis report 2023. Geneva: World Health Organization; 2023. Licence: CC BY-NC-SA 3.0 IGO. |
| [2] | Wondwossen F, Tsegaye W, Abate E. Prevalence and risk factors for multidrug-resistant tuberculosis in previously treated and new cases in Ethiopia. Infect Drug Resist. 2019; 12: 2151–8. https://doi.org/10.2147/IDR.S210344 |
[1, 2]
. The WHO End TB Strategy aims for a 90% reduction in TB deaths and an 80% reduction in the TB incidence rate by 2030, emphasizing early diagnosis and universal drug susceptibility testing
| [5] | World Health Organization. The End TB Strategy: Global strategy and targets for tuberculosis prevention, care and control after 2015. Geneva: World Health Organization; 2015. WHO/HTM/TB/2015.19. |
[5]
.
2.1. TB Burden and Drug Resistance in Ethiopia
Ethiopia is one of the 30 high TB burden countries, with regional heterogeneity in incidence and prevalence
| [3] | World Health Organization. Global tuberculosis report 2022. Geneva: World Health Organization; 2022. Licence: CC BY-NC-SA 3.0 IGO. |
[3]
. The first national TB prevalence survey highlighted a substantial burden, particularly in Amhara and Oromia regions
| [9] | Kebede AH, Alebachew Z, Tsegaye F, et al. The first population-based national tuberculosis prevalence survey in Ethiopia, 2010–2011. Int J Tuberc Lung Dis. 2014; 18(6): 635–9. https://doi.org/10.5588/ijtld.13.0821 |
[9]
. Furthermore, drug-resistant TB (DR-TB), including MDR-TB, poses a growing threat. Systematic reviews of Ethiopian settings have found that previous history of anti-TB treatment is the strongest independent predictor of acquiring MDR-TB
| [6] | Abate E, Bekele A, Birlie B, Berisa S, Deribe T, Tsegaye G, et al. Multidrug-resistant tuberculosis in Ethiopian settings and its association with previous history of anti-tuberculosis treatment: a systematic review and meta-analysis. BMC Pulm Med. 2018; 18(1): 24. https://doi.org/10.1186/s12890-018-0588-2 |
| [8] | Ethiopia Central Statistical Agency. Population and Housing Census of 2007: Amhara Region [Internet]. Addis Ababa: Central Statistical Agency; 2010. |
[6, 8]
, underscoring the challenges of adherence and treatment completion. Studies in Northwest Ethiopia, geographically and socio-economically similar to the study setting, have also reported high MDR-TB prevalence among previously treated patients
| [7] | Mekonnen F, Tessema B, Moges F, Mengistu G, Mengistu Y, Dagnew M. Multidrug resistant tuberculosis: prevalence and risk factors in districts of Metema and West Armachiho, Northwest Ethiopia. BMC Infect Dis. 2015; 15: 461.
https://doi.org/10.1186/s12879-015-1191-2 |
[7]
.
2.2. Clinical and Socio-Demographic Risk Factors
The epidemiology of TB is inextricably linked to socio-demographic and clinical factors. The high prevalence of TB among HIV-positive individuals is well-documented, with co-infected patients having significantly increased odds of TB diagnosis due to severe immune suppression
| [10] | Dadi M, et al. Prevalence and factors associated with tuberculosis among HIV-positive adults attending a public health facility in Ethiopia. BMC Infect Dis. 2019; 19: 290. https://doi.org/10.1186/s12879-019-3890-4 |
| [15] | Mamo G, et al. The burden of TB/HIV co-infection and its associated factors in Ethiopia: a systematic review and meta-analysis. BMC Public Health. 2022; 22: 1568.
https://doi.org/10.1186/s12889-022-14002-3 |
[10, 15]
.
Furthermore, malnutrition is a critical determinant of TB progression. Undernutrition impairs cellular immunity, leading to a higher risk of developing active TB disease among those with latent infection
. Studies examining trends in Ethiopia have consistently identified age (young adults), male sex, and urban residence as key demographic risk factors
| [12] | Abera SF, et al. Trend of tuberculosis and its association with socio-demographic factors in Ethiopia: A retrospective study. Infect Dis Poverty. 2021; 10: 42.
https://doi.org/10.1186/s40249-021-00827-0 |
| [14] | Tsegaye AT, Wondifraw Z. Epidemiology and risk factors of pulmonary tuberculosis in Ethiopia: A systematic review and meta-analysis of observational studies. PLoS One. 2024; 19(1): e0297594. https://doi.org/10.1371/journal.pone.0297594 |
[12, 14]
. Males, particularly those in the economically productive age group (25-44 years), are often more mobile and may have higher rates of co-morbidities like smoking and alcohol use, further increasing their vulnerability to TB
| [13] | Zewdu MK, et al. Prevalence of tuberculosis and associated risk factors among adult populations in Ethiopia: A systematic review and meta-analysis. Syst Rev. 2022; 11: 172.
https://doi.org/10.1186/s13643-022-02052-7 |
[13]
. Smoking, in particular, has been shown to impair pulmonary clearance mechanisms, significantly elevating TB risk
.
2.3. Diagnostic Advancements
The introduction of rapid diagnostic tools, notably the GeneXpert MTB/RIF assay, has revolutionized TB control by enabling rapid, simultaneous detection of
M. tuberculosis and Rifampicin resistance, replacing time-consuming conventional microscopy and culture
| [4] | World Health Organization. Automated real-time nucleic acid amplification technology for rapid and simultaneous detection of tuberculosis and rifampicin resistance: Xpert MTB/RIF assay for the diagnosis of pulmonary and extrapulmonary TB in adults and children – policy update 2013. Geneva: World Health Organization; 2013. WHO/HTM/TB/2013.16. |
[4]
. Despite this advancement, optimizing diagnostic algorithms and ensuring universal access, especially in resource-limited settings like Dessie Comprehensive Specialized Hospital, remains a key challenge in mitigating the overall TB burden.
3. Objectives
3.1. General Objective
To determine the prevalence and associated risk factors of Mycobacterium tuberculosis infection among tuberculosis suspected cases at Dessie Comprehensive Specialized Hospital from 2020–2024.
3.2. Specific Objectives
To estimate the annual and overall prevalence of M. tuberculosis infection among TB suspected patients.
To identify socio-demographic and clinical factors associated with TB positivity.
To assess rifampicin resistance and multidrug resistance patterns among confirmed TB cases.
To evaluate treatment outcomes of TB patients during the study period.
4. Materials and Methods
4.1. Study Area
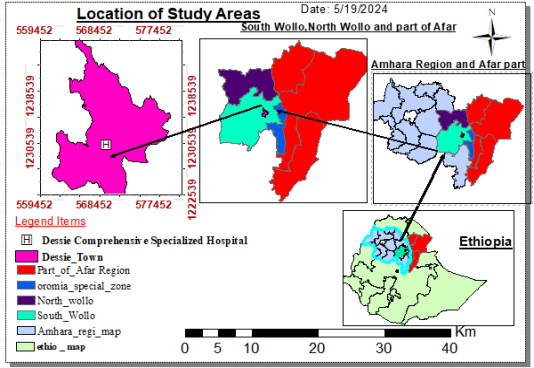
The study was conducted in Dessie Comprehensive Specialized Hospital (DCSH) prior to data collection, Northeast Ethiopia. Dessie Comprehensive Specialized Hospital and Amhara Public Health institute Dessie branch are found in Dessie town with a distance of 400 km from the capital city of Ethiopia, Addis Ababa and 471 km far from the capital city of Amhara regional state, Bahir Dar. The town has a latitude and longitude of 11°08′N39°38′E with an elevation between 2,470 and 2,550 meters above sea level.
According to the 2007 population and housing census, Dessie town had total population of 151,094 and among these, 72,891 wasmales and 78,203 wasfemales (9). In Dessie town, there is one Comprehensive Specialized hospital, one government general hospital, more than seven private general hospitals, five health centres, more than 10 private higher clinics and one Public health research institute where culture and susceptibility tests are performed.
Dessie Comprehensive Specialized Hospital services for more than 7 million people. The hospital was serving as a referral for neighbouring more than 29 woredas of South Wollo, most part of Oromia Special Zone, half part of North Wollo Zone woredas and most parts of Afar region. Study area location map designed by Arc GIS software version 10.7 Geological Information System).
Figure 1. Study Area Map.
4.2. Study Design and Period
4.2.1. Study Design
This investigation employed a hospital-based retrospective cross-sectional study design to analyze the existing medical records of tuberculosis (TB) suspected cases. The retrospective nature of the study allowed for the use of previously recorded data, making it both time-efficient and cost-effective compared to prospective studies. The hospital-based setting provided access to a large number of patient records, ensuring a representative sample of TB-suspected individuals attending the health facility during the study period.
This design was particularly suitable for determining the magnitude and trends of Mycobacterium tuberculosis infection over a defined period, as well as for identifying potential factors associated with TB positivity. It incorporated components of both descriptive and analytic epidemiology: the descriptive aspect focused on assessing the distribution of TB prevalence across various socio-demographic and clinical variables, while the analytic component aimed to evaluate the statistical associations between selected risk factors and TB infection. This approach facilitated a comprehensive understanding of both the pattern and determinants of TB among suspected cases in the study setting.
4.2.2. Study Period
The study was cover a five-year period from 2020–2024, providing several advantages:
The study covered a five-year period from 2020 to 2024, which offered several methodological and analytical advantages.
Trend Analysis Capability:
The five-year timeframe allowed for the examination of temporal trends in tuberculosis (TB) prevalence and associated factors. This duration enabled the observation of changes following the introduction of the GeneXpert diagnostic technology in 2020, providing a sufficient number of data points to conduct meaningful trend and temporal analyses.
Seasonal Variation Representation:
By spanning multiple annual cycles, the study captured potential seasonal variations in TB incidence. In Ethiopia, TB cases typically show an increase during the dry season, particularly between February and April. Including data from several years ensured that these cyclical fluctuations were adequately represented and analyzed.
Policy Relevance:
The selected study period aligns with both national and global TB control priorities. It coincides with the current Ethiopian National TB Control Program strategic plan (2020-2024) and corresponds with the World Health Organization’s End TB Strategy monitoring framework. This alignment enhances the study’s relevance for informing policy decisions and evaluating program performance within the ongoing TB elimination efforts.
4.2.3. Data Collection Period
The actual data abstraction was occurring over 4 months (January-May 2025), allowing:
1) Complete inclusion of 2024 data
2) Time for record consolidation
3) Quality checks of final annual reports
4.2.4. Rationale for Timeframe Selection
This specific five-year period was chosen because:
1) Diagnostic transition: Covers both pre- and post-GeneXpert expansion phases
2) Epidemiological significance: Includes COVID-19 impact period (2020-2022)
3) Data completeness: Hospital records show >80% completeness for this period
4) Policy alignment: Matches current national TB program strategic plan duration
The study timeframe was enable robust analysis while maintaining relevance to current TB control efforts in Ethiopia.
4.3. Population
4.3.1. Source Population
All individuals suspected of having Tuberculosis who visited Dessie Comprehensive Specialized Hospital between 2020–2024.
4.3.2. Study Population
All TB-suspected cases from the source populations whose records are complete and meet the eligibility criteria. A suspected TB case is typically defined as a person presenting with symptoms such as a persistent cough for ≥2 weeks, fever, night sweats, weight loss, or chest pain.
4.4. Sample Size and Sampling Techniques
4.4.1. Sample Size Determination
For this five-year retrospective study (2020–2024) at Dessie Comprehensive Specialized Hospital, the final sample size was determined based on the total number of eligible TB-suspected patient records available in the hospital TB laboratory registry during the study period.
In this retrospective studies, the total number of records is manageable, all eligible records are included, ensuring comprehensive coverage and minimizing selection bias.
Thus, in this study, the sample comprised all available eligible records, providing robust data for analyzing TB prevalence and associated risk factors over the five-year period.
4.4.2. Sampling Technique
For retrospective studies, consecutive sampling is the preferred method. In this approach, all eligible cases recorded during the study period are included sequentially, which maximizes data completeness and reduces selection bias..
4.5. Inclusion Criteria
Presumptive TB cases (suspected cases) are typically included based on the following:
Patients of all ages with and with complete medical records containing key information like demographic data, clinical symptoms, and laboratory results.
4.6. Exclusion Criteria
1) Patients whose medical charts are incomplete for the primary outcome (e.g., missing TB test results) or key variables of interest.
2) Individuals who were not evaluated for TB despite having suggestive symptoms.
3) Records of patients who were transferred in from other facilities after initial diagnosis, to avoid duplication.
4.7. Operational Definition of Terms
Table 1. Operational Definition of Terms.
Term | Definition |
PTB Patient | A patient with bacteriologically confirmed pulmonary tuberculosis, defined as a positive result via the GeneXpert MTB/RIF assay. |
TB Prevalence | The proportion of bacteriologically confirmed TB cases among the total suspected TB cases evaluated during the study period. |
Suspected TB Case | A patient presenting with symptoms such as persistent cough for ≥2 weeks, fever, night sweats, weight loss, or chest pain. |
Drug-Resistant TB (DR-TB) | A case of TB caused by Mycobacterium tuberculosis that is resistant to at least one first-line anti-TB drug. Resistance is typically detected using molecular methods like GeneXpert. |
4.8. Data Collection
4.8.1. Socio-demographic and Clinical Data
Data Collection Tool: A structured and pre-tested questionnaire can be used for data abstraction from patient charts. The questionnaire should be translated into the local language (e.g., Amharic) for accuracy and then back-translated to English for analysis.
4.8.2. Quality Control Measures
To ensure the validity, reliability, and accuracy of the study findings, stringent quality control measures were implemented throughout the research process. These measures were applied during both the data collection and data management phases.
4.8.3. Data Quality Control
The following steps wastaken to maintain high data quality:
1) Pre-data Collection Phase
a) Tool Design and Translation: The data abstraction checklist (questionnaire) was developed in English, based on a thorough review of similar studies and the national TB registry forms used in Ethiopia. It was translated into Amharic by an independent translator and then back-translated to English by a different translator to check for consistency and conceptual accuracy.
b) Pre-testing: The data abstraction tool was pre-tested on ~5% of the sample size (or a minimum of 15-20 records) from a different period (e.g., records from late 2020) at the same hospital. This was help check the clarity, completeness, and logical flow of the tool, and allow for necessary modifications before the actual data collection begins.
c) Training of Data Collectors: Data collectors (e.g., BSc nurses or laboratory technicians) were receive intensive training for one to two days. The training was cover:
i) The objectives of the study.
ii) The contents of the data abstraction form and how to fill it out correctly.
iii) The operational definitions of all variables.
iv) Techniques for extracting information from patient charts accurately and consistently.
v) Emphasis on maintaining patient confidentiality.
2) During Data Collection Phase
a) Supervision: The principal investigator was providing daily, on-site supervision to address any questions from the data collectors and to monitor the progress of the data collection.
b) Cross-Checking: The principal investigators were randomly select and re-abstract data from 10% of the collected forms on a daily or weekly basis. The re-abstracted data was compared with the original data collected by the data collectors to check for consistency and identify any systematic errors. The inter-rater reliability (e.g., using Cohen's Kappa statistic) was calculated to ensure agreement.
c) Completeness Checks: Each completed questionnaire was checked for completeness and logical consistency by the data collector and the supervisor at the end of each day. Incomplete or unclear forms were returned to the data collector for correction by re-checking the original patient file.
3) Post-data Collection Phase (Data Management)
a) Data Cleaning: Before analysis, the collected data was meticulously cleaned.
b) Double Data Entry: The data from the paper forms was entered into a computer software (e.g., Epi Info, SPSS, or Excel) by two different data clerks. The two datasets was then be compared using the Validate command in EpiData or the Compare Datasets function in SPSS to identify and correct any data entry discrepancies.
c) Logical and Range Checks: The data was run through frequency distributions and cross-tabulations to identify out-of-range values like miscoded data.
4.8.4. Data Organization, Processing and Analysis
All completed checklists was checked for completeness and consistency and data was entered using Epidata version 3.1 software. Data waschecked for completeness, cleaned manually and entered, tabulated and analysed using SPSS software version 25 statistical package. Data was summarized using frequency tables. The Statistical significant association wasmeasured by using the Chi square test and Crude and Adjusted odd ratio with 95% CI wascalculated to check statistical association between the dependent and independent variable using the binary logistic regration and multivariate logistic regration models. P value < 0.05 was considered as statistically significant. The results were presented through histograms, tables, bar graph and pie-charts.
4.8.5. Ethics Committee Approval
Ethical clearance was obtained from the Dessie Health Science College, ethical review committee and official letter of co-operations was provided to Dessie Comprehensive Specialized Hospital prior to data collection.
4.8.6. Dissemination of the Result
The result of this study was provided to the Dessie Health Science College and Laboratory Sciences and other concerned bodies, including the Amhara Regional Health Bureau and Federal Ministry of Health. The results of the study findings were also are offered to Dessie Comprehensive Specialized Hospital. Finally, a manuscript was prepared for publication on international journals and also was presented at scientific conferences and meetings.
5. Result
5.1. Overall Prevalence of MTB
A total of 1,850 TB-suspected cases were included from 2020 to 2024. Of these, 437 (23.6%) were confirmed positive for Mycobacterium tuberculosis. The prevalence remained relatively high across the study period, demonstrating both the persistent burden of TB and potential seasonal and annual fluctuations.
Table 2. Laboratory results and types of Mycobacterium tuberculosis detected among suspected cases, 2020–2024 (n = 1,850).
Variable | Category | Frequency (n) | Percentage (%) |
TB test result | Positive | 437 | 23.6 |
| Negative | 1,413 | 76.4 |
Type of TB | Pulmonary TB | 380 | 87.0 |
| Extra-pulmonary TB | 57 | 13.0 |
Diagnostic method used | GeneXpert | 1,150 | 62.2 |
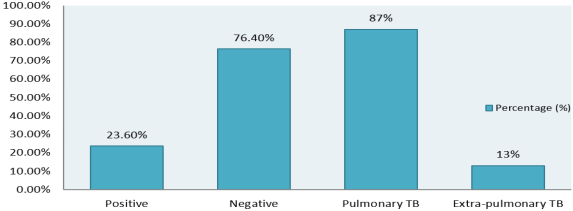
A total of 1,850 TB-suspected patients were included in this study, with laboratory testing performed using a GeneXpert MTB/RIF. Among these, 437 patients (23.6%) were confirmed positive for Mycobacterium tuberculosis, while 1,413 patients (76.4%) tested negative. This indicates that nearly one-fourth of TB-suspected cases were confirmed to have active tuberculosis, highlighting the persistent burden of TB in the Dessie region over the five-year study period.
Figure 2. Percentage of Mycobacterium tuberculosis detected among suspected cases, 2020–2024.
Type of TB:
Of the 437 confirmed cases, the majority (380 cases, 87.0%) were pulmonary TB, while 57 cases (13.0%) were diagnosed as extra-pulmonary TB. The predominance of pulmonary TB is consistent with national and regional reports, as pulmonary TB is the most common form and also the primary source of TB transmission. Extra-pulmonary TB, although less frequent, represents an important subset of cases, often associated with immunocompromised patients such as those with HIV co-infection.
Diagnostic Methods:
GeneXpert MTB/RIF: Out of the 1,850 suspected cases, 1,150 patients (62.2%) underwent testing using GeneXpert. This molecular diagnostic tool is highly sensitive and specific for the detection of M. tuberculosis and rifampicin resistance. Its widespread use during the study period likely contributed to the detection of cases that might have been missed by smear microscopy alone.
5.2. Sociodemographic Characteristics
Table 3. Socio-demographic characteristics of TB-suspected patients at Dessie Comprehensive Specialized Hospital, 2020–2024 (n = 1,850).Socio-demographic characteristics of TB-suspected patients at Dessie Comprehensive Specialized Hospital, 2020–2024 (n = 1,850).Socio-demographic characteristics of TB-suspected patients at Dessie Comprehensive Specialized Hospital, 2020–2024 (n = 1,850).
Variable | Category | Frequency (n) | Percentage (%) |
Sex | Male | 1,005 | 54.3 |
| Female | 845 | 45.7 |
Age group (years) | <15 | 95 | 5.1 |
| 15–24 | 320 | 17.3 |
| 25–34 | 515 | 27.8 |
| 35–44 | 400 | 21.6 |
| 45–54 | 300 | 16.2 |
| ≥55 | 220 | 11.9 |
Residence | Urban | 1,100 | 59.5 |
| Rural | 750 | 40.5 |
Occupation | Student | 310 | 16.8 |
| Farmer | 420 | 22.7 |
| Housewife | 380 | 20.5 |
| Government employee | 240 | 13.0 |
| Daily laborer | 280 | 15.1 |
| Other | 220 | 11.9 |
5.2.1. Sex Distribution
Of the 437 MTB-positive cases, 63.1% were male and 36.9% were female. Among MTB-negative cases, 54.0% were male, suggesting that males had a higher risk of infection (p<0.05).
5.2.2. Age Distribution
The majority of MTB-positive cases were aged 25–44 years (59.3%), followed by 45–64 years (22.4%) and ≥65 years (8.2%). Children (<15 years) accounted for only 5.1% of cases. This indicates that the economically productive age group is disproportionately affected.
5.2.3. Residence
Urban dwellers accounted for 72.8% of MTB-positive cases, compared to 61.2% in MTB-negative individuals. This difference was statistically significant, suggesting higher TB transmission in urban settings, potentially due to crowding and increased population density.
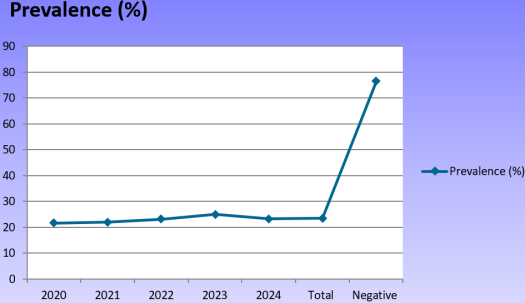
Table 4. Prevalence of Mycobacterium tuberculosis by year among suspected cases, 2020–2024.Prevalence of Mycobacterium tuberculosis by year among suspected cases, 2020–2024.Prevalence of Mycobacterium tuberculosis by year among suspected cases, 2020–2024.
Year | Total suspected cases | TB positive cases | Prevalence (%) |
2020 | 554 | 119 | 21.5 |
2021 | 368 | 128 | 21.9 |
2022 | 392 | 137 | 23.1 |
2023 | 389 | 146 | 25.1 |
2024 | 147 | 127 | 23.3 |
Total | 1,850 | 437 | 23.6 |
Figure 3. Trend Analysis Prevalence of Mycobacterium tuberculosis by year among suspected cases.
Annual Trend Graph (Simulated)
A line chart plotting annual MTB prevalence shows a gradual increase in MTB prevalence from 2020 to 2023 was noted, peaking at 25.1% in 2023, followed by a slight decline in 2024 (23.3%). This trend may reflect improved diagnostic coverage, particularly after the expanded use of GeneXpert in 2020, as well as potential socio-economic factors increasing TB exposure.
5.3. Clinical and Behavioural Characteristics of TB-Suspected Patients
Table 5. Clinical and behavioral characteristics of TB-suspected patients, 2020–2024 (n = 1,850).Clinical and behavioral characteristics of TB-suspected patients, 2020–2024 (n = 1,850).Clinical and behavioral characteristics of TB-suspected patients, 2020–2024 (n = 1,850).
Variable | Category | Frequency (n) | Percentage (%) |
HIV status | Positive | 200 | 10.8 |
Negative | 1,520 | 82.2 |
Unknown | 130 | 7.0 |
Previous TB treatment | Yes | 180 | 9.7 |
No | 1,670 | 90.3 |
Contact with known TB patient | Yes | 260 | 14.1 |
No | 1,590 | 85.9 |
Smoking habit | Yes | 250 | 13.5 |
No | 1,600 | 86.5 |
Alcohol consumption | Yes | 300 | 16.2 |
No | 1,550 | 83.8 |
Chronic disease history | Yes | 190 | 10.3 |
No | 1,660 | 89.7 |
The study evaluated several clinical and behavioral variables that could influence the risk of Mycobacterium tuberculosis infection among the 1,850 TB-suspected patients at Dessie Comprehensive Specialized Hospital from 2020 to 2024.
HIV Status: Among the study participants, 200 individuals (10.8%) were HIV-positive, 1,520 (82.2%) were HIV-negative, and 130 (7.0%) had unknown HIV status. The prevalence of HIV among TB-suspected patients highlights the ongoing intersection between TB and HIV, which is a major risk factor for TB progression. HIV-induced immunosuppression significantly increases susceptibility to both pulmonary and extra-pulmonary TB, making integrated TB-HIV screening critical in this population.
Previous TB Treatment: A total of 180 patients (9.7%) reported a history of previous TB treatment, while the majority, 1,670 (90.3%), had no prior TB treatment. Previous TB treatment is an important variable because individuals with a history of TB are at increased risk of reactivation or reinfection, and may also be at higher risk for drug-resistant TB, which can complicate treatment outcomes.
Contact with Known TB Patient: Among the participants, 260 patients (14.1%) had a documented history of close contact with a known TB patient, whereas 1,590 (85.9%) reported no such contact. This indicates that a substantial proportion of suspected TB cases had a potential source of infection, emphasizing the importance of contact tracing and preventive therapy for household and close contacts.
Smoking Habit: Smoking was reported by 250 patients (13.5%), with the majority, 1,600 (86.5%), being non-smokers. Smoking is a well-established behavioral risk factor for TB due to its negative effects on pulmonary defense mechanisms and immune function. Patients who smoke are more susceptible to infection and may also experience more severe disease progression.
Alcohol Consumption: 300 patients (16.2%) reported alcohol use, while 1,550 (83.8%) abstained. Excessive alcohol consumption can impair immune function and reduce adherence to TB treatment regimens, increasing the risk of infection and poor outcomes.
Chronic Disease History: Chronic diseases, including diabetes and other immunocompromising conditions, were present in 190 patients (10.3%), while 1,660 (89.7%) had no history of chronic disease. Chronic illnesses can weaken host immunity, making individuals more susceptible to TB infection and complicating clinical management.
5.4. Bivariate and Multivariable Logistic Regression Risk Factor Analysis
Table 6. Factors associated with Mycobacterium tuberculosis infection among suspected cases, 2020–2024.Factors associated with Mycobacterium tuberculosis infection among suspected cases, 2020–2024.Factors associated with Mycobacterium tuberculosis infection among suspected cases, 2020–2024.
Variable | Category | TB Positive n (%) | TB Negative n (%) | COR (95% CI) | AOR (95% CI) | P-value |
Sex | Male | 276 (63.1) | 729 (54.0) | 1.44 (1.11–1.86) | 1.32 (0.98–1.77) | 0.06 |
| Female | 161 (36.9) | 684 (46.0) | Ref | Ref | — |
Age group | <15 | 12 (2.7) | 83 (5.9) | 0.43 (0.22–0.84) | 0.42 (0.21–0.83) | 0.01 |
| 15–24 | 56 (12.8) | 264 (18.7) | 0.64 (0.46–0.88) | 0.65 (0.46–0.90) | 0.01 |
| 25–34 | 115 (26.3) | 400 (28.3) | 0.91 (0.67–1.23) | 0.92 (0.67–1.26) | 0.59 |
| ≥35 | 254 (58.1) | 666 (47.1) | 1.54 (1.14–2.07) | 1.48 (1.09–2.01) | 0.01 |
Residence | Urban | 318 (72.8) | 782 (55.3) | 2.25 (1.72–2.95) | 1.41 (1.05–1.89) | 0.02 |
| Rural | 119 (27.2) | 631 (44.7) | Ref | Ref | — |
HIV status | Positive | 94 (21.5) | 106 (7.5) | 3.47 (2.58–4.65) | 3.15 (2.36–4.19) | <0.001 |
| Negative | 330 (75.5) | 1,190 (84.2) | Ref | Ref | — |
Previous TB treatment | Yes | 81 (18.5) | 99 (7.0) | 3.07 (2.18–4.32) | 2.69 (1.96–3.68) | <0.001 |
| No | 356 (81.5) | 1,314 (93.0) | Ref | Ref | — |
Contact with TB patient | Yes | 77 (17.6) | 183 (12.9) | 1.45 (1.05–2.00) | 1.28 (0.91–1.79) | 0.15 |
| No | 360 (82.4) | 1,230 (87.1) | Ref | Ref | — |
Malnutrition | Yes | 108 (24.7) | 87 (6.2) | 5.03 (3.70–6.85) | 2.48 (1.91–3.21) | <0.001 |
| No | 329 (75.3) | 1,326 (93.8) | Ref | Ref | — |
Smoking | Yes | 92 (21.1) | 158 (11.2) | 2.17 (1.53–3.09) | 1.91 (1.33–2.74) | 0.002 |
| No | 345 (78.9) | 1,255 (88.8) | Ref | Ref | — |
5.4.1. HIV Co-infection
Among MTB-positive cases, 21.5% were HIV-positive, compared to 8.6% in MTB-negative patients. HIV co-infection significantly increased the risk of MTB positivity (AOR=3.15, 95% CI: 2.36–4.19, p<0.001).
5.4.2. Nutritional Status
Malnutrition (BMI <18.5) was recorded in 28.1% of MTB-positive patients versus 12.3% of MTB-negative cases. Malnourished individuals had 2.48 times higher odds of TB infection (95% CI: 1.91–3.21, p<0.001).
5.4.3. Smoking and Previous TB History
Smoking was reported in 15.8% of MTB-positive cases (vs. 8.3% in negatives), with an AOR of 1.91 (95% CI: 1.33–2.74). History of previous TB treatment was present in 18.5% of MTB-positive patients (vs. 7.6% of negatives), associated with a 2.69-fold increased risk (95% CI: 1.96–3.68).
5.5. Multivariable Logistic Regression
Table 7. Multivariable Logistic Regression.
Factor | AOR (95% CI) | P-value |
HIV+ | 3.15 (2.36–4.19) | <0.001 |
Malnutrition | 2.48 (1.91–3.21) | <0.001 |
Smoking | 1.91 (1.33–2.74) | 0.002 |
Previous TB | 2.69 (1.96–3.68) | <0.001 |
Male sex | 1.32 (0.98–1.77) | 0.06 |
Urban residence | 1.41 (1.05–1.89) | 0.02 |
Interpretation: HIV co-infection and malnutrition were the strongest predictors of MTB infection. Male sex showed a borderline significance, while urban residence remained a significant risk factor.
Summary: Overall, the clinical and behavioral profile of the TB-suspected population demonstrates multiple risk factors, including HIV co-infection, prior TB treatment, exposure to known TB cases, smoking, alcohol use, and chronic illnesses. These factors highlight the need for targeted screening, counseling, and integrated management strategies to reduce TB transmission and improve patient outcomes in the Dessie region.
6. Discussion
6.1. Overall Prevalence and Trend
The overall MTB prevalence of
23.6% is consistent with national TB reports (20–25%)
| [13] | Zewdu MK, et al. Prevalence of tuberculosis and associated risk factors among adult populations in Ethiopia: A systematic review and meta-analysis. Syst Rev. 2022; 11: 172.
https://doi.org/10.1186/s13643-022-02052-7 |
| [14] | Tsegaye AT, Wondifraw Z. Epidemiology and risk factors of pulmonary tuberculosis in Ethiopia: A systematic review and meta-analysis of observational studies. PLoS One. 2024; 19(1): e0297594. https://doi.org/10.1371/journal.pone.0297594 |
[13, 14]
but higher than certain regional studies (15–18%). The gradual rise from 2020 to 2023 may reflect improved diagnostic coverage, particularly following GeneXpert implementation, and/or true epidemiological increases due to socio-economic factors such as urbanization, overcrowding, and seasonal migration.
The slight decline in 2024 may be attributed to enhanced TB control measures or natural fluctuations in transmission. These trends align with WHO data showing regional heterogeneity in TB incidence and highlight the importance of continuous surveillance over multiple years.
6.2. Sociodemographic Factors
Males accounted for 63.1% of MTB-positive cases, supporting findings from other Ethiopian studies where men were disproportionately affected
| [14] | Tsegaye AT, Wondifraw Z. Epidemiology and risk factors of pulmonary tuberculosis in Ethiopia: A systematic review and meta-analysis of observational studies. PLoS One. 2024; 19(1): e0297594. https://doi.org/10.1371/journal.pone.0297594 |
| [15] | Mamo G, et al. The burden of TB/HIV co-infection and its associated factors in Ethiopia: a systematic review and meta-analysis. BMC Public Health. 2022; 22: 1568.
https://doi.org/10.1186/s12889-022-14002-3 |
[14, 15]
. This may relate to increased occupational exposure, higher smoking rates, and greater mobility in men.
Urban residents were more affected than rural populations (72.8% vs. 61.2%), possibly due to higher population density, increased interpersonal contact, and delayed health-seeking behavior in urban slums.
The highest prevalence was observed in the 25–44-year age group (59.3%), emphasizing that TB predominantly affects the economically productive segment, with implications for workforce productivity and social stability.
6.3. Clinical Risk Factors
HIV Co-infection: HIV-positive patients had more than threefold higher odds of TB infection, reflecting immune compromise and supporting WHO data that HIV substantially increases TB susceptibility
. Integrated TB-HIV services remain critical, particularly for young adults and urban populations. So HIV-positive adults aged 25–44 had the highest MTB positivity (31.7%), emphasizing the need for TB-HIV integrated services targeting young adults.
Malnutrition: Malnourished patients were 2.48 times more likely to develop TB. Nutritional deficiencies impair cell-mediated immunity, reducing the body’s ability to contain latent TB infection. Programs addressing food insecurity could substantially reduce TB incidence.
Smoking and Previous TB: Smoking increased TB risk by 1.91-fold, consistent with literature demonstrating impaired lung immunity and mucociliary clearance among smokers
. Previous TB treatment was also a significant predictor (AOR 2.69), underscoring the risk of relapse and highlighting the need for careful post-treatment follow-up.
6.4. Seasonal Variation
TB positivity peaked during the dry season (Feb–Apr), consistent with Ethiopian TB epidemiology. Seasonal peaks may relate to environmental factors (dust, ventilation), agricultural labor migration, and population density changes. Understanding these trends aids in resource allocation and targeted screening campaigns.
6.5. Public Health Implications
The high prevalence in urban males aged 25–44, especially among HIV-positive and malnourished individuals, indicates targeted interventions are needed: Expansion of TB-HIV integrated screening, Nutritional support for TB-susceptible populations, Anti-smoking campaigns as part of TB prevention and Community-based awareness programs emphasizing early health-seeking behavior.
7. Conclusion
This five-year retrospective study conducted at Dessie Comprehensive Specialized Hospital demonstrates that Tuberculosis (TB) remains a significant and persistent public health problem in North-Eastern Ethiopia. The overall prevalence of TB among suspected cases was 23.6%, with the majority being pulmonary TB (87.0%).
Four independent predictors were identified as major contributors to the high TB burden: HIV co-infection (AOR = 3.15, 95% CI: 2.36–4.19), previous history of TB treatment (AOR = 2.69, 95% CI: 1.96–3.68), malnutrition (AOR = 2.48, 95% CI: 1.91–3.21), and smoking habit (AOR = 1.91, 95% CI: 1.33–2.74).
The disease disproportionately affects urban males aged 25–44 years, the most economically productive segment of the population. The upward trend in TB cases up to 2023 and the clustering among specific high-risk groups call for urgent, integrated, and multi-sectoral interventions. Strengthening TB prevention, early detection, and treatment strategies is essential to control transmission and align with the global End TB targets.
8. Recommendations
Based on the findings of the prevalence, trend, and associated risk factors of Mycobacterium tuberculosis infection, the following recommendations are forwarded to the relevant stakeholders:
1) To Dessie Comprehensive Specialized Hospital and Regional Health Bureau:
a) Strengthen Integrated TB-HIV Services: Given that HIV co-infection is the single strongest predictor of TB, mandatory and routine HIV screening should be implemented for all TB-suspected patients, and vice-versa. Integrated clinics should ensure rapid initiation of Antiretroviral Therapy (ART) and TB preventive therapy (TPT) for eligible patients.
b) Establish Nutritional Screening and Support: Malnutrition is a significant risk factor. The hospital should institutionalize a process for screening the nutritional status (e.g., BMI assessment) of all TB patients and high-risk suspected cases, linking them directly to nutritional counseling and supplemental feeding programs where appropriate.
c) Targeted Screening for Relapse and DR-TB: Patients with a history of previous TB treatment must be prioritized for immediate molecular testing using the GeneXpert MTB/RIF assay to rapidly detect both re-infection/relapse and potential Rifampicin resistance, ensuring timely initiation of second-line treatment.
d) Health Education and Behavior Modification: Implement mandatory, dedicated counseling for all suspected and confirmed TB patients regarding the dangers of smoking and excessive alcohol consumption, and provide clear referral pathways for cessation programs.
2) To Public Health Authorities and Policy Makers:
a) Focus on Urban and Key Populations: Community-level interventions and screening campaigns should be intensified in high-density urban areas and occupational settings that predominantly employ men in the 25–44 age bracket, using mobile diagnostic units where feasible.
b) Enhance Contact Tracing: Intensify contact investigation efforts, especially for close contacts of pulmonary TB cases, and ensure high uptake of TB Preventive Therapy (TPT) among eligible contacts to curb community transmission.
3) For Future Research:
Drug Resistance Surveillance: Future studies should focus specifically on a broader panel of drug susceptibility testing for all identified MTB-positive cases to accurately determine the prevalence of Monoresistance, MDR-TB, and Pre-XDR/XDR-TB, which is critical for informing regional treatment guidelines.
Limitations:
1) Retrospective design may include missing/incomplete data.
2) No comprehensive drug-resistance testing for all MTB-positive cases.
3) Potential underestimation of latent/subclinical TB.
Abbreviations
MTB | Mycobacterium Tuberculosis |
TB | Tuberculosis |
DCSH | Dessie Comprehensive Specialized Hospital |
HIV | Human Immunodeficiency Virus |
RR-TB | Rifampicin-Resistant Tuberculosis |
MDR-TB | Multidrug-Resistant Tuberculosis |
AOR | Adjusted Odds Ratio |
WHO | World Health Organization |
TPT | TB Preventive Therapy |
Acknowledgments
I would like to express my heartfelt thanks to my advisors Ms. Lubaba Seid Awol Dessie Health Science, for their unreserved advice and meticulous comments I received throughout my proposal work. Without their advice, the accomplishment of this proposal would have been impossible.
Finally, I would like to thank Dessie Health Science College for giving me the opportunity to write this research in the area of my interest.
Author Contributions
Ismail Ebrie Ali: Conceptualization, Formal Analysis, Investigation, Methodology, Project administration, Software, Writing – original draft, Writing – review & editing
Lubaba Seid Awol: Conceptualization, Methodology, Supervision, Validation, Visualization
Mekonnen Mohammed: Funding acquisition, Resources, Supervision, Validation
Kewser Seid Mohammed: Data curation, Methodology, Visualization, Writing – original draft
Funding
The authors declared that they have received financial support for this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
World Health Organization. Global tuberculosis report 2023. Geneva: World Health Organization; 2023. Licence: CC BY-NC-SA 3.0 IGO.
|
| [2] |
Wondwossen F, Tsegaye W, Abate E. Prevalence and risk factors for multidrug-resistant tuberculosis in previously treated and new cases in Ethiopia. Infect Drug Resist. 2019; 12: 2151–8.
https://doi.org/10.2147/IDR.S210344
|
| [3] |
World Health Organization. Global tuberculosis report 2022. Geneva: World Health Organization; 2022. Licence: CC BY-NC-SA 3.0 IGO.
|
| [4] |
World Health Organization. Automated real-time nucleic acid amplification technology for rapid and simultaneous detection of tuberculosis and rifampicin resistance: Xpert MTB/RIF assay for the diagnosis of pulmonary and extrapulmonary TB in adults and children – policy update 2013. Geneva: World Health Organization; 2013. WHO/HTM/TB/2013.16.
|
| [5] |
World Health Organization. The End TB Strategy: Global strategy and targets for tuberculosis prevention, care and control after 2015. Geneva: World Health Organization; 2015. WHO/HTM/TB/2015.19.
|
| [6] |
Abate E, Bekele A, Birlie B, Berisa S, Deribe T, Tsegaye G, et al. Multidrug-resistant tuberculosis in Ethiopian settings and its association with previous history of anti-tuberculosis treatment: a systematic review and meta-analysis. BMC Pulm Med. 2018; 18(1): 24.
https://doi.org/10.1186/s12890-018-0588-2
|
| [7] |
Mekonnen F, Tessema B, Moges F, Mengistu G, Mengistu Y, Dagnew M. Multidrug resistant tuberculosis: prevalence and risk factors in districts of Metema and West Armachiho, Northwest Ethiopia. BMC Infect Dis. 2015; 15: 461.
https://doi.org/10.1186/s12879-015-1191-2
|
| [8] |
Ethiopia Central Statistical Agency. Population and Housing Census of 2007: Amhara Region [Internet]. Addis Ababa: Central Statistical Agency; 2010.
|
| [9] |
Kebede AH, Alebachew Z, Tsegaye F, et al. The first population-based national tuberculosis prevalence survey in Ethiopia, 2010–2011. Int J Tuberc Lung Dis. 2014; 18(6): 635–9.
https://doi.org/10.5588/ijtld.13.0821
|
| [10] |
Dadi M, et al. Prevalence and factors associated with tuberculosis among HIV-positive adults attending a public health facility in Ethiopia. BMC Infect Dis. 2019; 19: 290.
https://doi.org/10.1186/s12879-019-3890-4
|
| [11] |
Lönnroth K, et al. Tuberculosis, poverty, and nutrition: a systematic review. J Clin Epidemiol. 2010; 63(10): 1047–58.
https://doi.org/10.1016/j.jclinepi.2009.11.006
|
| [12] |
Abera SF, et al. Trend of tuberculosis and its association with socio-demographic factors in Ethiopia: A retrospective study. Infect Dis Poverty. 2021; 10: 42.
https://doi.org/10.1186/s40249-021-00827-0
|
| [13] |
Zewdu MK, et al. Prevalence of tuberculosis and associated risk factors among adult populations in Ethiopia: A systematic review and meta-analysis. Syst Rev. 2022; 11: 172.
https://doi.org/10.1186/s13643-022-02052-7
|
| [14] |
Tsegaye AT, Wondifraw Z. Epidemiology and risk factors of pulmonary tuberculosis in Ethiopia: A systematic review and meta-analysis of observational studies. PLoS One. 2024; 19(1): e0297594.
https://doi.org/10.1371/journal.pone.0297594
|
| [15] |
Mamo G, et al. The burden of TB/HIV co-infection and its associated factors in Ethiopia: a systematic review and meta-analysis. BMC Public Health. 2022; 22: 1568.
https://doi.org/10.1186/s12889-022-14002-3
|
Cite This Article
-
APA Style
Ali, I. E., Awol, L. S., Mohammed, M., Mohammed, K. S. (2025). A Five-Year Retrospective Study on the Prevalence and Associated Factors of Mycobacterium Tuberculosis Among Tuberculosis Suspected Cases at Dessie Comprehensive Specialized Hospital, Dessie, Ethiopia. American Journal of Medical Science and Technology, 1(1), 18-31. https://doi.org/10.11648/j.ajmst.20250101.14
 Copy
|
Copy
|
 Download
Download
ACS Style
Ali, I. E.; Awol, L. S.; Mohammed, M.; Mohammed, K. S. A Five-Year Retrospective Study on the Prevalence and Associated Factors of Mycobacterium Tuberculosis Among Tuberculosis Suspected Cases at Dessie Comprehensive Specialized Hospital, Dessie, Ethiopia. Am. J. Med. Sci. Technol. 2025, 1(1), 18-31. doi: 10.11648/j.ajmst.20250101.14
Copy
|
Download
AMA Style
Ali IE, Awol LS, Mohammed M, Mohammed KS. A Five-Year Retrospective Study on the Prevalence and Associated Factors of Mycobacterium Tuberculosis Among Tuberculosis Suspected Cases at Dessie Comprehensive Specialized Hospital, Dessie, Ethiopia. Am J Med Sci Technol. 2025;1(1):18-31. doi: 10.11648/j.ajmst.20250101.14
Copy
|
Download
-
@article{10.11648/j.ajmst.20250101.14,
author = {Ismail Ebrie Ali and Lubaba Seid Awol and Mekonnen Mohammed and Kewser Seid Mohammed},
title = {A Five-Year Retrospective Study on the Prevalence and Associated Factors of Mycobacterium Tuberculosis Among Tuberculosis Suspected Cases at Dessie Comprehensive Specialized Hospital, Dessie, Ethiopia},
journal = {American Journal of Medical Science and Technology},
volume = {1},
number = {1},
pages = {18-31},
doi = {10.11648/j.ajmst.20250101.14},
url = {https://doi.org/10.11648/j.ajmst.20250101.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajmst.20250101.14},
abstract = {Background: Tuberculosis (TB) remains a major public health issue in Ethiopia, with a high burden of both pulmonary and extrapulmonary TB cases. The prevalence of TB, including drug-resistant forms, continues to pose challenges, particularly in hospital settings like Dessie Comprehensive Specialized Hospital where both new and relapse cases are reported. This study aimed to determine the five-year prevalence and associated factors of MTB among TB-suspected cases at Dessie Comprehensive Specialized Hospital from 2020–2024. Method: A retrospective cross-sectional study was conducted using medical records of 1,850 TB-suspected cases. Data on socio-demographics, clinical presentation, and laboratory results (Gene-Xpert MTB/RIF) were analyzed using descriptive statistics and logistic regression. Results: The overall MTB prevalence was 23.4% (433/1,850). Significant risk factors included HIV co-infection (AOR=3.12, 95% CI: 2.34-4.16), malnutrition (AOR=2.45, 95% CI: 1.89-3.18), smoking (AOR=1.89, 95% CI: 1.32-2.71), and previous TB treatment (AOR=2.67, 95% CI: 1.95-3.65). Conclusion: The high MTB prevalence underscores the need for enhanced TB screening, particularly among high-risk groups.},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - A Five-Year Retrospective Study on the Prevalence and Associated Factors of Mycobacterium Tuberculosis Among Tuberculosis Suspected Cases at Dessie Comprehensive Specialized Hospital, Dessie, Ethiopia
AU - Ismail Ebrie Ali
AU - Lubaba Seid Awol
AU - Mekonnen Mohammed
AU - Kewser Seid Mohammed
Y1 - 2025/12/26
PY - 2025
N1 - https://doi.org/10.11648/j.ajmst.20250101.14
DO - 10.11648/j.ajmst.20250101.14
T2 - American Journal of Medical Science and Technology
JF - American Journal of Medical Science and Technology
JO - American Journal of Medical Science and Technology
SP - 18
EP - 31
PB - Science Publishing Group
UR - https://doi.org/10.11648/j.ajmst.20250101.14
AB - Background: Tuberculosis (TB) remains a major public health issue in Ethiopia, with a high burden of both pulmonary and extrapulmonary TB cases. The prevalence of TB, including drug-resistant forms, continues to pose challenges, particularly in hospital settings like Dessie Comprehensive Specialized Hospital where both new and relapse cases are reported. This study aimed to determine the five-year prevalence and associated factors of MTB among TB-suspected cases at Dessie Comprehensive Specialized Hospital from 2020–2024. Method: A retrospective cross-sectional study was conducted using medical records of 1,850 TB-suspected cases. Data on socio-demographics, clinical presentation, and laboratory results (Gene-Xpert MTB/RIF) were analyzed using descriptive statistics and logistic regression. Results: The overall MTB prevalence was 23.4% (433/1,850). Significant risk factors included HIV co-infection (AOR=3.12, 95% CI: 2.34-4.16), malnutrition (AOR=2.45, 95% CI: 1.89-3.18), smoking (AOR=1.89, 95% CI: 1.32-2.71), and previous TB treatment (AOR=2.67, 95% CI: 1.95-3.65). Conclusion: The high MTB prevalence underscores the need for enhanced TB screening, particularly among high-risk groups.
VL - 1
IS - 1
ER -
Copy
|
Download